
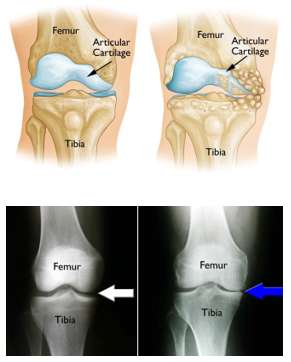
 Osteoarthritis can develop when the bones of your knee and leg do
not line up properly. This can put extra stress on either the inner
(medial) or outer (lateral) side of your knee. Over time, this extra
pressure can wear away the smooth articular cartilage that protects the
bones, causing pain and stiffness in your knee.
Osteoarthritis can develop when the bones of your knee and leg do
not line up properly. This can put extra stress on either the inner
(medial) or outer (lateral) side of your knee. Over time, this extra
pressure can wear away the smooth articular cartilage that protects the
bones, causing pain and stiffness in your knee.
Osteotomy
literally means “cutting the bone.” The main goal of Osteotomy is to
change the alignment of the limb in order to decrease the load on the
affected side of the limb (either medial or lateral) and thereby
decrease the pain associated with arthritis and improve function, as
well as slow the progression of arthritis.
Knee osteotomy is
used when a patient has early-stage osteoarthritis that has damaged just
one side of the knee joint. It is usually done for patients who are
younger and are more active than those requiring
knee
replacements. In a knee osteotomy, either the tibia (shinbone) or
femur (thighbone) is cut and then reshaped to relieve pressure on one of
the compartments (which is worn to a higher degree) of the knee joint.
By shifting weight off of the damaged side of the joint, an osteotomy
can relieve pain and significantly improve function in an
arthritic knee. This is done by creating a controlled fracture,
most commonly in the tibia (shin bone) just below the knee or
occasionally the femur (thigh bone) just above the knee. The alignment
of the knee can thus be altered, and by doing this, the weight on the
worn part of the joint is decreased, and is transferred more to the less
worn areas.
Knee osteotomy has three goals:
- To transfer weight from the arthritic part of the knee to a healthier area
- To correct poor knee alignment
- To prolong the life span of the knee joint
One advantage of the procedure is that, by preserving your own knee anatomy, a successful osteotomy may delay the need for a joint replacement for several years. Another advantage is that there are no restrictions on physical activities after an osteotomy-you will be able to participate in your favorite activities, even high-impact exercise.
Osteotomy does have disadvantages. For example, pain relief is not as predictable after osteotomy compared with a partial or total knee replacement. And recovery from osteotomy is typically longer and more difficult because you may not be able to bear weight on your operated knee right away. In some cases, having had an osteotomy can make later knee replacement surgery more challenging. Because results from total knee replacement and partial knee replacement have been so successful, knee osteotomy has become less common. Nevertheless, it remains an option for many patients.
Procedure
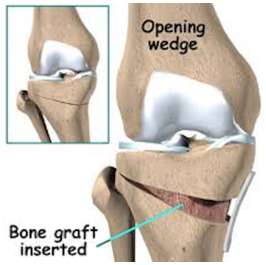 In a tibial osteotomy, a wedge of bone is removed to straighten out the leg. Most osteotomies for knee arthritis are done on the tibia (shinbone) to correct a bowlegged alignment that is putting too much stress on the inside of the knee. During this procedure, a controlled fracture is created on the inner side of the tibia, under the worn-out side of the knee. When the surgeon opens the fracture into a wedge, it straightens the leg. This brings the bones on the worn-out side of the knee apart and creates more space between the bones on the damaged, arthritic side. The artificially created fracture gap is filled autologous bone graft or bone graft substitutes. As a result, the knee is loaded on the unaffected side and can carry weight more evenly, easing pressure on the painful side. Tibial osteotomy was first performed in Europe in the late 1950s and in the United States in the 1960s. This procedure is sometimes called a "high tibial osteotomy” Osteotomies of the thighbone (femur) are done using the same technique. They are usually done to correct a knock-kneed alignment.
In a tibial osteotomy, a wedge of bone is removed to straighten out the leg. Most osteotomies for knee arthritis are done on the tibia (shinbone) to correct a bowlegged alignment that is putting too much stress on the inside of the knee. During this procedure, a controlled fracture is created on the inner side of the tibia, under the worn-out side of the knee. When the surgeon opens the fracture into a wedge, it straightens the leg. This brings the bones on the worn-out side of the knee apart and creates more space between the bones on the damaged, arthritic side. The artificially created fracture gap is filled autologous bone graft or bone graft substitutes. As a result, the knee is loaded on the unaffected side and can carry weight more evenly, easing pressure on the painful side. Tibial osteotomy was first performed in Europe in the late 1950s and in the United States in the 1960s. This procedure is sometimes called a "high tibial osteotomy” Osteotomies of the thighbone (femur) are done using the same technique. They are usually done to correct a knock-kneed alignment.
Candidates for Knee Osteotomy
Knee osteotomy is most effective for thin, active patients who are less than 60 years old. Good candidates have pain on only one side of the knee, and no pain under the kneecap. Knee pain should be brought on mostly by activity, as well as by standing for a long period of time. Candidates should be able to fully straighten the knee and bend it at least 90 degrees. Patients with rheumatoid arthritis are not good candidates for osteotomy. Your orthopaedic surgeon will help you determine whether a knee osteotomy is suited for you.
Before Surgery
You are admitted to hospital on the day of surgery and will see Dr. Chirag Patel and your anaesthetist prior to surgery. Please bring all of you X-Ray and scans with you to hospital. Also ensure that you have no cuts or scratches on your skin, as this is an infection risk, and will usually result in surgery being deferred. Your anaesthetist will discuss with you the kind anaesthesia that will be administered to you. The leg alignment is usually changed by cutting the tibia (shin bone) just below the knee. A knee osteotomy operation typically lasts between 1 and 2 hours.
The Surgery
Your surgeon will make an incision at the inner side of your knee, starting below your kneecap. He or she will plan out the correct size of the wedge using guide wires. With an oscillating saw, your surgeon will cut along the guide wires. The bone cut is then opened up based on your pre-operative scannogram alignment using highly specialised sequential devices. After creating the gap and checking the alignment, a wedge of bone is inserted to fill the gap. This wedge is either taken from the pelvis, or artificial bone graft substitutes can be used. Dr. Chirag will discuss this with you preoperatively. The position is then held with a plate and screws, a drain may be inserted prior to closing the wound and a brace applied is applied post-operatively. After the surgery, you will be taken to the recovery room where you will be closely monitored as you recover from the anaesthesia. You will then be taken to your hospital room.
Complications
As with any surgical procedure, there are risks involved with osteotomy. Your surgeon will discuss each of the risks with you and will take specific measures to help avoid potential complications. Although the risks are low, the most common complications include:
- Infection: Bony infection is very rare but if this occurs and is untreated, serious problems follow.
- Blood clots: Meditation and stockings are used to help prevent clots.
- Injuries to vessels and nerves: Major nerves and arteries which supply the leg are in the vicinity of the surgery. Although rare, damage to these Is possible.
- Other complications: These include, superficial infection and knee stiffness.
- Failure of the osteotomy to heal: In appropriately 2 - 3% of patient, the bone may not fully heal or slip in position whilst healing. This is monitored by x-ray of the bone. Occasionally revision surgery may be required to promote bone healing.
Pain management & Discharge
After surgery, you will feel some pain, but our team will make every effort to help you feel as comfortable as possible. Recovery and hospital discharge in most patients is planned for 1 to 2 days after an osteotomy.
Weight bearing
After the operation, you will most likely need to use crutches for several weeks. You will be advised to wear a knee brace for 6 weeks, and use crutches for 12 weeks. An x-ray is taken at 6 weeks to healing of the bone, prior to gradually increasing the weight you put on your leg. During the second 6 weeks you will be gradually allowed to bear weight and increase the weight on your leg, whilst remaining protected with mobility aides.
Doctor visit
You will see Dr. Chirag Patel for a follow-up visit 7 days after surgery and again two weeks after the surgery for a surgical wound. X-rays may be taken so that he can check how well the osteotomy has healed. After the follow-up, your surgeon will tell you when it is safe to put weight on your leg, and when you can start rehabilitation.
Rehabilitation exercises
Rehabilitation with the physiotherapist is commenced 6 weeks after surgery when the healing of the bone is progressing. This is aimed at restoring your movement and muscle strength. During rehabilitation, a physical therapist will give you exercises to help maintain range of motion in your knee and restore the muscle strength in the operated limb. It takes most patients about 6 months to fully recover from high tibial osteotomy surgery. It is possible to resume sedentary job approximately 3 to 4 weeks after surgery, if this can be done on the crutches. It is usually at least 3 to 4 months before physical work is possible and between 6 to 12 months before sports can be resumed depending upon the rate of bone healing. You are strongly advised to be compliant with the therapy prescribed by the physical therapist in order gain maximum from the high tibial osteotomy surgery.
Outcome
For most patients (more than 90%), osteotomy is successful in relieving pain and delaying the progression of arthritis in the knee. It can allow a younger patient to lead a more active lifestyle for many years. Even though many patients will ultimately require a
total knee replacement, an osteotomy can be an effective way to buy time until a replacement is required.
Tibial osteotomy usually results in good pain relief and improvement in function. There is no cure for arthritis, and osteotomy does not reverse arthritis but should slow its rapid progression. Osteotomy is typically used in the young or active patient (less than 50) where the arthritis is not in an advanced stage, whereas old less than active patients would more commonly undergo knee replacement.
The wisdom of performing an osteotomy is that it will allow the native knee to survive longer. The older a patient is at the time of the knee replacement, the more likely the replacement will last the patient the remainder of their life. Replacing a knee in a patient who has had prior tibial osteotomy may be slightly more difficult than performing a primary knee replacement. Most patients feel improvement in their knee following tibial osteotomy. A few (5-8%) are unimproved and 2% are worse. The improvement seen following tibial osteotomy lasts a variable time depending on how well the patient cares for the knee as well as the degree of damage already done by arthritis, and the inherited quality of the articular cartilage in the joint. For over 70% of the improvement following osteotomy lasts for 10 years or more.
If you have any question concerning your surgery is risk, benefits, likely outcome or complication please do not hesitate to contact a team member at Joint & Sports Clinic.