Carpal tunnel syndrome is a common condition of the wrist joint that causes pain, numbness, and tingling in the hand. The condition occurs when one of the major nerves to the hand, the median nerve is squeezed or compressed as it travels through the wrist. In most patients, carpal tunnel syndrome gets worse over time, so early diagnosis and treatment are important.
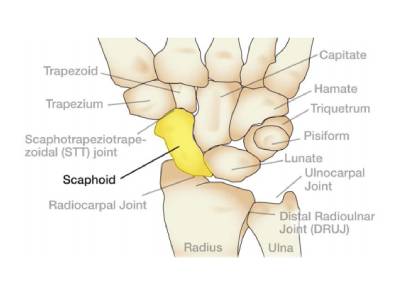
The wrist joint lie between the two forearm bones (the radius on the thumb side and the ulna on the little finger side) and the digital rays of the finger where they origin from the forearm. The wrist joint is made of two rows of 4 bones each called the carpal bones and arranged in succession between the forearm bones and the metacarpal bones.
Radiocarpal joint: This joint is where the radius, one of the forearm bones, joins with the first row of wrist bones (scaphoid, lunate, and triquetrum).
Ulnocarpal joint: This joint is where the ulna, the other forearm bone, joins with the lunate and triquetrum wrist bones. This joint is commonly injured when you sprain your wrist.
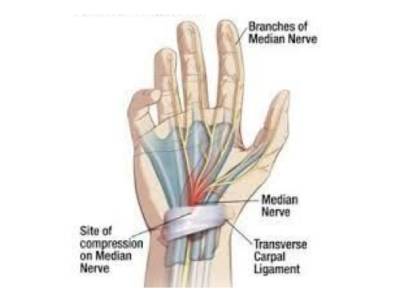
The carpal tunnel is a narrow passageway in the wrist, about an inch wide. The floor and sides of the tunnel are formed by the wrist or the carpal bones. The roof of the tunnel is a strong band of connective tissue called the transverse carpal ligament. Because these boundaries are very rigid, the carpal tunnel has little capacity to "stretch" or increase in size.
The median nerve is one of the main nerves in the hand. It originates as a group of nerve roots in the neck. These roots come together to form a single nerve in the arm. The median nerve goes down the arm and forearm, passes through the carpal tunnel at the wrist, and goes into the hand. The nerve provides the sensations instructions from the thumb, index and middle finger to the brain as well as movement instructions from the brain to the thumb and index, middle, and ring fingers. There are nine tendons that bend the fingers and thumb which travel through the carpal tunnel. These tendons are called flexor tendons. The inner surface of the carpal tunnel is lined by a thin tissue called the synovium
Carpal tunnel syndrome occurs when the tunnel becomes narrowed or when tissues surrounding the flexor tendons (synovium) swell, putting pressure on the median nerve. Normally, the synovium lubricates the tendons, making it easier to move your fingers.
When the synovium swells, it takes up space in the carpal tunnel and, over time, crowds the nerve. This abnormal pressure on the nerve can result in pain, numbness, tingling, and weakness in the hand and is called as the carpal tunnel syndrome.
Most cases of carpal tunnel syndrome are caused by a combination of factors. Studies show that women and older people are more likely to develop the condition. Some of the risk factors for carpal tunnel syndrome include
Symptoms of carpal tunnel syndrome may include:
In most cases, the symptoms of carpal tunnel syndrome begin gradually without a specific injury. Many patients find that their symptoms come and go at first. However, as the condition worsens, symptoms may occur more frequently or may persist for longer periods of time. Night-time symptoms are very common. Because many people sleep with their wrists bent, symptoms may awaken you from sleep. During the day, symptoms often occur when holding something for a prolonged period of time with the wrist bent forward or backward, such as when using a phone, driving, or reading a book. Many patients find that moving or shaking their hands helps relieve their symptoms.
During your evaluation, your doctor will talk to you about your general medical history and will ask about your symptoms. He or she will carefully examine your hand and wrist and perform a number of physical tests. During these tests, your doctor will:
Based on the physical examination and your clinical history, your doctor may strongly suspect the diagnose the carpal tunnel syndrome. There are certain test that your surgeon may order to confirm the diagnosis or when the physical examination does not correlate with your clinical history.
For most people carpal tunnel syndrome will worsen over time without some form of treatment. For this reason, it is important to be evaluated and diagnosed by your doctor early on. In the early stages, it may be possible to slow or stop the progression of the disease. If neglected however, there is a potential for the median nerve to be damaged irreversibly.
If diagnosed and treated early, the symptoms of carpal tunnel syndrome can often be relieved without surgery. If your symptoms are mild, your doctor will recommend nonsurgical treatment first. Nonsurgical treatments may include:
The decision whether to have surgery is based on the severity of your symptom. In long-standing cases with constant numbness and wasting of your thumb muscles, surgery may be recommended to prevent irreversible damage. If nonsurgical treatment does not relieve your symptoms after a period of time, your doctor may recommend surgery
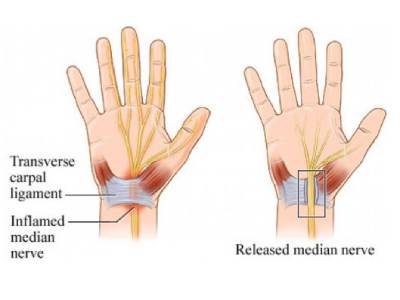
The surgical procedure performed for carpal tunnel syndrome is called a "carpal tunnel release.” The goal of the surgery is to relieve pressure on your median nerve by cutting the ligament that forms the roof of the tunnel. This increases the size of the tunnel and decreases pressure on the median nerve. As the ligament heals, there is more room for the nerve and tendons
In most cases, carpal tunnel surgery is done on an outpatient basis. The surgery can be done under regional anesthesia, which numbs the affected arm along with sedation which puts you to sleep, or under local anesthesia, which numbs just your hand and wrist.
Your doctor makes a small incision in the palm of your hand and views the inside of your hand and wrist through this incision. During the procedure, your doctor will divide the transverse carpal ligament (the roof of the carpal tunnel). This increases the size of the tunnel and decreases pressure on the median nerve. After surgery, the ligament gradually grows back together, but there will be more space in the carpal tunnel and pressure on the median nerve will be relieved. The carpal tunnel can also be released minimally invasively and is called as endoscopic carpal tunnel release. The outcomes of open surgery and endoscopic surgery are similar. There are benefits and potential risks associated with both techniques. Your doctor will talk with you about which surgical technique is best for you.
Immediately following surgery, you will be advised to elevate your hand above your heart and move your fingers to reduce swelling and prevent stiffness. There may be some pain, swelling, and stiffness after your procedure. Minor soreness in your palm may last for several weeks to several months. You may have to wear a splint or wrist brace for several weeks. You will, however, be allowed to use your hand for light activities, taking care to avoid significant discomfort. Driving, self-care activities, and light lifting and gripping may be permitted soon after surgery.
However, the muscle strength is inversely related to the damage to the median nerve, i.e. lesser the damage to the nerve, better is the muscle strength. Hence patients should bear in mind that grip and pinch strength usually return by about 2 to 3 months as the median nerve recovers from the pressure injury after surgery. If the condition of your median nerve was poor before surgery, however, grip and pinch strength may not improve for about 6 to 12 months. Your doctor will talk with you about when you will be able to return to work and whether you will have any restrictions on your work activities.
As with any surgical procedure, complications may occur with carpal tunnel syndrome, however the chance are rare. Your doctor will take steps to minimize the risks of complications. Some of the most common complications of carpal tunnel release surgery include:
For most patients, surgery will improve the symptoms of carpal tunnel syndrome. Recovery, however, may be gradual and complete recovery may take up to a year. In long-standing cases of carpal tunnel syndrome with severe loss of feeling and/or muscle wasting around the base of the thumb, recovery will be slower and may not be complete in comparison to the opposite normal hand. Occasionally, carpal tunnel syndrome can recur, although this is rare. If this happens, you may need additional treatment or surgery
